Comprehensive information about colorectal cancer, also called bowel cancer, colon cancer or rectal cancer, including symptoms, causes and alternative colorectal cancer treatments from berberine and artemisinin to Keytruda and Proton Beam Therapy.
Colorectal cancer (CRC), Colon cancer, Rectal cancer, Bowel cancer
Colorectal cancer may variously be called bowel cancer, colon cancer, rectal cancer or CRC. So everything below may be described as
- bowel cancer information,
- colon cancer information,
- rectal cancer information, or
- colorectal cancer (CRC) information
Take your pick.
This comprehensive cancer information overview and associated articles will help you increase your personal odds of beating colorectal cancer - the symptoms, the diagnosis and all the latest cancer options on cancer treatments and therapies - from cancer drugs and chemotherapy to surgery, radiotherapy and complementary cancer therapies, and even alternative colorectal cancer therapies; including all the very latest alternative treatments and emerging new therapies and information. We will even cover the causes and colorectal cancer prevention.
Understanding Colorectal Cancer
Up front, it is important to talk of the advances made in very recent years in our understanding of the contributing factors to the disease and its spread.
For example:
1. Gut imbalance, gut bacteria and particularly the mRNA of pathogens has been clearly linked to colorectal cancer. The SYNCAN study in Europe and work from 'Microbiome Otago' at the University of Otago, New Zealand, have shown that there are three different forms of Colorectal cancer. Each involves a group of pathogens, each 'gang' is led by a pathogen, Fusobacterium, and E.coli is a major player in all. However, gang members differ. There is also a loss of important strains such as a Clostridium strain that manages sugar. And further up the gut can be areas with normal bacteria present.
You need to address problems in the gut microbiome in order to stand any chance of getting fully better. As we will see the herb Artemisinin can play a big role.
Go to: How Gut bacteria play a role in colorectal cancer
2. Spreading the cancer through surgery: It is often written that metastases seem to occur at a very early stage in this cancer. However, it could well be that spread may be worsened by surgery since the surgeon cannot know exactly where the bad bacteria end and the healthy gut starts again. There is evidence of the use of anti-histamines like Cimetidine being used from one week after surgery for at least a year, and contributing to a doubling of survival times. This is because cancer cells have more histamine receptor sites, and histamines encourage their inflammation and stickiness.
Go to: How to reduce the threat of surgery spreading colorectal cancer
3. The crucial importance of sugar: There is also clear evidence that common sugar is a colorectal cancer driver. Indeed, research from Weill Cornell shows that one can of fizzy soft drink a day increases colorectal cancer tumour size. Not surprisingly then, the blood-sugar-reducing drug metformin helps bowel cancer survival as does the herb berberine, which inhibits colorectal metastases. Other complementary therapies have been shown to help survival, like curcumin, fish oil omega-3, and probiotics, even fecal enemas, whereas antibiotics have been shown to hinder. This really is a cancer where integrative medicine is important.
Go to: Sugar drives colorectal cancer
The causes of colorectal cancer
Colorectal cancer is also referred to as Colon Cancer, Rectal cancer or Bowel cancer. Traditionally, it was more common in people over 60 especially men, although there has been a growing trend towards more occurrence in younger adults, with increases in sub-groups for example, in younger, pregnant women.
In the UK colorectal cancer (CRC, or bowel cancer) is the third most common cancer for men and the second most common cancer for women. Globally, the picture is similar.
Although there were some claims in a CRUK report that a better diet nowadays is producing a reduction in this cancer in the UK, we can find little evidence of that in the figures. If anything the total number of cases of this disease is rising, especially in the young.
There is no cancer more linked to disturbances in the gut. Without a shadow of doubt, this cancer has been linked to the over-use of antibiotics and to food-poisoning especially in younger adults as they travel the world:
Go to: Colorectal cancer linked to taking antibiotics
Go to: All cancer begins in the gut
Go to: Are antibiotics the cause of the growth of Colorectal cancer in the young
And the truth is that a modern poor diet, along with modern lifestyle factors such as smoking, obesity, inactivity (and even increasing diabetes levels which have been linked to increased risk), are also making this cancer a great deal more prevalent. But this, again, is because a modern diet high in sugar and alcohol, but low in soluble fibre, fruits, and vegetables is encouraging a poor microbiome in the gut.
In the EU, 6% of men and women may be affected by the age of 75. Western Europeans may be particularly susceptible due to the combination of inherited risk (of polyps, for example) and a diet often high in fat and low in fibre (de Ferlay et al 2001; Gill & Rowland 2002).
The official causes of Colorectal cancer?

The official causes are polyps (growths) in the colon or rectum; hereditary pre-disposition; a diet high in fat; or Crohn's disease and Ulcerative Colitis (Medline USA). Other risk factors include smoking, inactivity, heavy alcohol consumption and obesity. People diagnosed with Diabetes have three times the risk.
-
Crohn's Disease (also called: Enteritis, Ileitis ) causes inflammation of the digestive system. It is just one of a group of diseases called IBS, or inflammatory bowel disease. The disease can affect any area from the mouth to the anus, although it is more commonly found in the lower part of the small intestine called the ileum. Crohns disease seems to run in some families. It can occur in people of all age groups but is most often diagnosed in young adults. Common symptoms include weight loss, joint pain, skin problems, fever, pain in the abdomen and bloody diarrhoea. The disease can lead to blockages and even malnutrition. Research has indicated the involvement of certain gut bacteria especially after a bout of food poisoning:
Go To: Gut bacteria, Crohns and Colorectal Cancer
-
Ulcerative Colitis (also called: Colitis, Distal colitis, Pancolitis, Ulcerative proctitis) is a disease that causes ulcers in the lining of the colon and rectum. It is another form of IBS. In extreme cases where the inflammation causes severe inflammation and even cell death, ulcers can form. The disease can happen at any age usually starting between the ages of 15 and 30. It tends to run in families. The most common symptoms are anaemia, severe tiredness, pain in the abdomen, and even bloody diarrhoea.
Antibiotic intake, parasites, pathogens and a loss of commensal gut bacteria are now a major focus. Commensal bacteria (the good guys) produce short chain esters - one sodium butyrate - even kills colorectal cancer cells. Increasingly, colorectal cancer patients are supplementing with sodium butyrate.
Go to: The role of gut bacteria in colorectal cancer
Above all, the herb artemisinin, which can kill certain parasites, pathogens and yeasts, is attracting attention, especially as it has shown promise in killing colorectal cancer cancer cells and reducing tumour size. Herbs like artemisinin, curcumin and berberine are major components of an Integrative Treatment Plan in CRC.
Go to: Three studies show artemisinin has benefits in colorectal cancer
Go to: Berberine and cancer
Symptoms and Diagnosis of colorectal cancer
 Early diagnosis can lead to a greater chance of successful surgery
Early diagnosis can lead to a greater chance of successful surgery
When colorectal cancer is diagnosed early there is a much greater chance of successful surgery and cure. However, many individuals with colon cancer have no symptoms until the disease reaches an advanced stage, after metastasising (spreading) to other organs. (Most commonly to the liver, lungs and/or brain). Symptoms include continuous stomach cramps for six weeks, changed stool habit especially diarrhoea or constipation - for a similar period, bright red blood in the stool, and unexplained weight loss.
In more severe cases a blockage can occur with resulting symptoms of a bloated feeling, loss of appetite, constipation, pain and nausea.
Colorectal cancer symptoms; and screening
Screening methods include:
-
Stool blood test looking for signs of irregularities in the stools.
-
Sigmoidoscopy using a light an/or camera joined to a tube to check the rectum and lower colon. Where a camera is used simultaneous pictures may be observed on a TV monitor. As this only examines the lower bowel areas a small scraping of cells (a biopsy) is sometimes taken so that they can be examined under a microscope.
-
Colonoscopy using a small light and camera attached to a longer, very flexible tube and connected to a TV monitor to examine the whole colon. This will need to be empty for the examination, so dietary advice (including a total diet in the last day) is given. Laxatives, and sometimes even a total flush may be used. A few cells may be scraped away as a biopsy for examination.
-
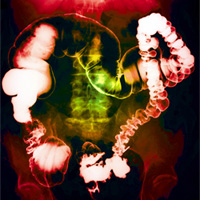
Barium enema This involves taking X-Rays of your intestine after a white chalky liquid is pumped through a tube inserted in your rectum. It is important that the intestine is clear, so you will be given laxatives, asked not to eat or drink in the preceding 12 hours and you may even have a tube inserted in your rectum so that warm water may be used to flush out the area for examination.
-
CEA assay where the amount of an antigen CEA is measured in the blood. This antigen is released in heightened levels if colon cancer cells are present and a test is used in the USA. Meanwhile, researchers in Giessen Hospital, Germany have confirmed that Pyruvate Kinase levels are also closely predictive of bowel cancer.
-
Lymph node biopsy where tissue samples of adjoining lymph nodes are studied under a microscope to see if there is spread.
-
Genetic screening if you have a strong family history of colo-rectal cancer you might consider a blood test to look for certain at risk genetic factors. The most common genetic factors occur in 2 conditions: hereditary nonpolyposis colorectal cancer (HNPCC, now called Lynch syndrome), an inherited disorder with increased risk for several types of cancer; and familial adenomatous polyposis (FAP), an inherited disorder linked to the formation of polyps inside the colon that may eventually become cancerous.
-
Sometimes further scans are used, most usually is there is some concern over spread of the cancer, or the doctors are just not obtaining a clear image. For example:
-
 Ultrasound - where a gel is used on your tummy, then a (why is it always so cold?) metal rod is simply passed over the top. Images show on a nearby screen.
Ultrasound - where a gel is used on your tummy, then a (why is it always so cold?) metal rod is simply passed over the top. Images show on a nearby screen.
- CT scan where a number of X-rays are taken to build up a 3D computer picture of whole areas of the body. You will be given an injection and your doctor should discuss allergies, asthma and iodine concerns with you before hand. (NB: Too many CT scans should be avoided where possible. Research from Columbia University (icon Vol 3 Issue 4) calculated that the radiation produced from an annual CT scan risks a 1 in 50 chance of death. The risks of a full body scan are reasonably well quantified says Dr David Brenner)
- MRI scan - similar to a CT scan, this uses magnetism rather than X-rays. You may be given an injection of a dye. No metal objects (necklaces, pacemakers, metal plates from former operations) are allowed.
- Chest X-Ray a normal X-ray to see if there is any spread to the lungs.
Colorectal Cancer staging
Different staging systems are used in different English speaking countries. Ask your doctor what stage you have and what exactly this means.
Stage 1 is localised in the bowel wall
Stage 2 is where it has spread through the muscle to the outer lining
Stage 3 is where it has moved into the lymph nodes
Stage 4 is where it has moved to other tissues in the body.
There is a system called Dukes decreasingly used in the US and UK. The above stages would be Dukes A, B, C and D respectively.
On the TNM system the first and second stages would be T, the third N and the last M.
Colorectal Cancer Treatment options
 Surgery: You may just have polyp removal during a colonoscopy.
Surgery: You may just have polyp removal during a colonoscopy.
Endoscopy may remove larger polyps and some of the bowel lining.
Where the cancer is in its early stages, surgery may just be enough to clear the cancer out of your intestines. Then, with an improved lifestyle and sensible monitoring, you can hope to remain cancer-free for a very long time, if not forever.
Surgery may also be used to clear blockages.
Since you may have one or more cancerous locations, you must ask your surgeon in advance exactly how much (in percentage terms) of your intestine he thinks he will be removing. And whether he will be taking lymph nodes as well from surrounding areas.
CRC and a stoma - You may also be given a stoma - a bag. You need to be very careful in advance of surgery. Ask about this possibility. If they are going to give you one, at what point in time do they plan to reverse it. A stoma is not just inconvenient. Your good diet will suffer greatly as the doctors will not want you to eat much fibre. You will be eating refined rubbish for several months.
There is clear evidence, although no phase III clinical trial as yet, that taking Cimetidine (Tagamet), a common antihistamine for a few days before, during and after surgery can restrict metastases. This was discovered by accident in 2002, when people co-incidentally taking the antihistamine, survived much longer after surgery.
Go to: Antihistamines increase survival in Colorectal cancer surgery
Cimetidine seems to stop cancer cells sticking to each other, and to the walls of blood vessels. It can also boost T-lymphocyte levels. The drugs benefits were found by accident - Integrative Practitioners suggest that it is taken from a few days before surgery to up to two years afterwards. Preliminary Clinical Trials showed a doubling of survival rates.
Chemotherapy: Chemotherapy may be given in advance of surgery in some cases of colon or rectal cancers, where the surgeon would like the tumour shrunk prior to removal (Neoadjuvant chemotherapy). It may also be given after surgery - to mop up any cancer cells in the blood or still in the gut (Adjuvant chemotherapy).
However, it is most usually given when the cancer has passed across the muscle tissue and there is risk of spread, or when spread has occurred already. Drugs commonly used are Fluorouracil (5-FU), oxaliplatin, capecitabine, gemcitabine, mitomycin, and irinotecan. Combinations of these are called FOLFOX and FOLFIRI.
Monoclonal antibodies are in development as a treatment too. Your doctor should be able to give you detailed information sheets on these drugs, and their side effects. You can also access our kiddies guide to drugs by going to the Treatments section of this Website and looking under chemotherapy.
There are more and more 'Targeted drugs', for example: Avastin, Erbitux, Vectibix, Cyramza, Stivarga and Zaltrap. These can be taken on their own or in conjunction with the chemo.
Then there is immunotherapy: The main two used are Pembrolizumab (Keytruda) and Nivolumab (Opdivo).
Liver Secondaries: You should look at our article on secondary Liver cancer. If you have concerns please ensure that you are taking adequate vitamin K supplementation. Vitamin K has been shown to reduce and even stop liver cancer growth. (Washington University, and Tokyo Medical School). But vitamin K is produced by the action of beneficial bacteria in the intestine. If you have taken drugs and your intestine is impaired it is very likely that you will not be making and absorbing adequate levels of vitamin K.
Radiotherapy: Rarely used for colon cancer because of the dangers to other nearby organs. Sometimes it is used with rectal cancers. You can find a useful article on how to get the most out of Radiotherapy in the Treatments section of this Website.
Proton Beam Therapy is increasingly used in the USA as it avoids the damage to secondary organs.
US experts are adamant: You should keep taking your vitamins especially antioxidants and fish oils and vitamin D they improve success rates of radiotherapy.
Diet, exercise and colorectal cancer survival
1. High blood sugar levels linked to lower colorectal cancer survival
As early as 2005 Johns Hopkins Kimmel Center were showing that poor blood sugar control (and diabetes) were risk factors for developing colorectal cancer. Further studies by that Center and elsewhere (especially the European SYNCAN study), have shown that Colorectal cancer goes hand in hand with the loss of a strain of Clostridium - a friendly strain that binds excess sugar in the gut and excretes it. Further studies have shown the importance of restricting glucose and fructose with colorectal cancer patients. In 2009, Johns Hopkins showed that "Colorectal Cancer may yield to sugar starvation". Metformin - the sugar lowering Diabetes drug - has been shown to increase CRC survival times in patients with diabetes. But it has also been shown to increase overall survival in any Colorectal cancer patient, even those without Diabetes. Similarly, the herb Berberine has also shown the same blood sugar-lowering and survival benefits. Berberine has been shown to inhibit the invasion and metastases of colorectal cancer cells.
Go to: Berberine and cancer
2. Saturated fat linked to lowered colorectal cancer survival
In people with cancer, fat can build up in the liver. Once it exceeds your personal fat threshold it then passes into the blood and lymph, and can even cause a fatty pancreas. A huge amount of work has been done on this by Professors Taylor and Leen, who are reversing type-2 diabetes
The problem is that high levels of bad fat and triglycerides in the blood stream are linked to more metastases and lowered survival.
Go To: Metastases increase the higher your saturated fat levels
Saturated fat is thus linked to lowered survival. A Rainbow Diet with its high good fat content, whole-food fibre and low sugar is therefore essential.
Go to: The Rainbow Diet
3. Diet and exercise crucial to survival in CRC
Rather like the CANCERactive guidelines on Diet and exercise, the American Cancer Society set out to show that theirs did deliver an increased survival. Taking colorectal cancer patients who had stage 3 disease and had undertaken both surgery and chemo, the ACS followed participents for 7 years. They found that those people who most closely followed diet and exercise guidelines survived 33 per cent longer and had 42 per cent less deaths in the 7 years.
One study showed that people who ate a lot of nuts survived CRC longer!
Go to: CANCERactive Guidelines on Diet and exercise
4. Vitamin D supplementation increases CRC survival times
Several studies have shown low vitamin D plasma levels in people on diagnosis with Colorectal Cancer. Levels should be around 100 ng/ml. Other studies have shown that taking drugs (Folfox, Folfiri, chemotherapy) can significantly reduce vitamin D levels in the body.
However there is research with CRC that shows vitamin D supplementation increases survival times. Without adequate vitamin D levels, the immune system is rendered ineffective. Boston Medical School suggest daily supplementation with 5,000IUs of vitamin D. People taking chemotherapy might like to double that dose.
Go to: Vitamin D supplementation increases CRC survival
5. Beware anaemia reducing survival times
Managing and counteracting anaemia can reduce death from anaemia by 50 per cent. Research published by the Cochrane Collaboration showed that epoetins (alfa and beta epoetin) show significant survival benefits. Particularly striking were the results for patients with solid tumours (Breast, lung, colon) where risk of death decreased by 51 per cent). In a second study (European Soc. For Medical Oncology - 31st Oct 2005) epotin beta was shown to reduce risk of tumour progression in patients with anaemia
Other Useful Information
UCLA Berkeley has a wellness letter (http://www.wellnessletter.com/) available to subscribers for free. Their sister journal from Johns Hopkins Cancer Center features colon cancer and will send you regular alerts.
people who had taken multivitamins at least 4 times per week had 30 per cent less risk of colon cancer
The American Cancer Society reported in 2003 on a study that ran from 1992 to 1997, looking at over 148,000 and their use of multi-vitamins. Those who had taken multivitamins during the 1980s at least 4 times per week had 30 per cent less risk of colon cancer. This was thought due to addition of vitamin D and folic acid in multivitamins.
One study shows that colorectal cancer patients survive longer if they regularly consume nuts!
Several studies from Germany and the USA have noted that Turmeric or Curcumin (See Nutritionals section of this website) is highly potent in the prevention and treatment of colon cancer.
Science (2005, 308) reports on the role played by parasites in colon cancer. Apparently increased colon cell activity is reported in order to displace the parasites, and this causes increased production of certain cytokines, interleukin, and interferon, all of which were associated with higher levels of the cancer.
A study involving 148,610 men and women in the USA between 50 and 74 years of age (Journal of the American Medical Assn) confirmed that the group who consumed most red meat had 30-40 per cent more distal colon or rectal cancer risk, when compared to the lowest consumers.
those with the highest magnesium levels had the lowest risk of colorectal cancer
A study from the Karolinska Institute, Sweden amongst 61,000 women showed that those with the highest magnesium levels had the lowest risk of colorectal cancer (40 per cent of adults are known to be magnesium deficient).
French scientists at the French National Institute for Health and Medical Research in Strasbourg have shown that procyanadins and polyphenols in apples help to prevent colon cancers. Other research studies have shown benefits for similar polyphenols in green tea and olive oil.
In the Boston Nurses Study, which finished in the mid 1990s after more than a decade of study, HRT was implicated in increased breast cancer risk. After further analysis longer-term use was implicated in other oestrogen-driven cancers like ovarian. Birmingham University (2001) showed that colon cancers were driven by localised oestrogen and this seems to be borne out by research from Wang at British Columbia, who in November 2004 looking at stomach/intestinal cancers, came out with a revolutionary new theory on cancer formation that it was due to the effect of oestrogen on stem cells from the bone marrow. Traditional theories almost always involve genetic mutation of cells. Here Wang was saying that your healing cells rushed round to repair inflammatory damage in your stomach/intestine but under the influence of oestrogen, they did not convert to normal healthy cells but stayed as rapidly dividing cells cancer cells because of the presence of oestrogen.
Irritation and Inflammation a precursor to colorectal cancer
Inflammation in the gut can be caused three ways.
1. By having the wrong gut bacteria and eating the wrong foods - it's a simple equation. Eat good foods - soluble fibres like pulses, vegetables, nuts and seeds and oats, psyllium - and you feed your commensal gut bacteria (the good guys) putting their numbers up dramatically. Your immune system will grow in proportion. However, eat bad foods like chocolate, sugar, fizzy soft drinks, refined foods, cows' dairy, gluten and you will increase the numbers of yeasts and pathogens in the gut and they will make more toxins and more inflammatory compounds. Which do you want?
Other good foods include berries, extra virgin olive oil and fish oils - these give you excesses of bacteria that make short-chain esters which reduce inflammation. One such ester is sodium butyrate which can kill colorectal cancer cells.
2. Chemicals can cause inflammation in the gut - outside factors, like toxic chemicals, smoking and binge drinking can directly alter the pH of the gut (as can stress) reducing levels of good bacteria. This allows the pathogens and the yeasts to come out to play.
3. Cox-2 is an enzyme in every cell of your body. Turn it on and it make inflammatory localised hormones. In 1982 John Vane won his Nobel Prize for the finding that aspirin could reduce the level of harmful eicosanoids (localised inflammatory hormones produced at the cellular level and lasting barely one and a half seconds). Cox-2 has a strong action in the gut. It increases the formation and aggression of polyps. Steroids, insulin and stress hormones turn it on. Research on fish oils by Leeds University Medical School showed they could calm and reduce the size of polyps and prevent CRC returning.
Turmeric (or curcumin) can deal with microbes and have a calming effect on Cox-2. As can berberine, which also reduces blood sugar.
One effect of these eicosanoids is to cause inflammation and irritation particularly the formation and growth of polyps; this can occur via this eicosanoid pathway, and/or via the consumption of animal fats which increases levels of inflammatory secondary bile fats. These plus inflammatory compounds from bad gut bacteria can increase polyp formation and bowel inflammation. Conversely, vitamin D, long-chain omega 3 (fish oils) and sodium butyrate can reduce this.
A great number of studies have also shown that garlic, ginger and salicylin (aspirin) can have a significan benefit. Aloe Vera is also known to be very calming. All seem to reduce Cox-2 inflammation.
Research shows that low magnesium levels are also a risk factor. However, 40% of people in the Westrn World are low in magnesium.
Is there a Role for Probiotics, Parasite killers and yeast killers in CRC?
There most certainly is! A good probiotic needs to have several strains of Lactobacillus, especially L. rhamnosus, which influences the volumes of the other bacteria in the gut and also plugs the holes in the gut wall created by yeasts.
It also needs several strains of Bifidobacterium, especially B. infantis, shown to help hugely with IBS and other stomach problems.
Research on artemisinin is quite clear that parasites can be a problem and you should look for a good parasite killer. It would be helpful if it also dealt with yeasts as antibiotics during surgery and chemotherapy can cause yeast infections which must be tackled.
Go to: Probiotics and Parasite killers to restore gut health
Let's be very clear. People who have had food poisoning get higher levels of pathogens in their gut, more illnesses like Crohn's and more colorectal cancer.
People who have taken antibiotics, especially as children, especially for prolonged periods of time (over 10 days) get more CRC. People who take drugs, especially drugs such as PPIs like omeprazole also severely damage their microbiome.
Go abroad a pick up a parasite and it affects the whole composition of the gut.
You should try to regenerate a healthy microbiome as fast as possible. We have a very important and easy to read book on this subject. It contains a very clear guide on how to heal your microbiome. It is essential reading.
Go to: Heal you Gut - Heal your Body
For people with a family history it is very important to go for an annual check even a regular endoscopy. The UK Government has been promising to bring these in on the NHS as a serious prevention weapon for several years now.
Complementary Colorectal cancer therapies; Alternative Colorectal cancer therapies?
CANCERactive is Europe's Number 1 Integrative Cancer Charity. This website alone has more than 4,000 pages of information on it, either as articles or as news stories. More than 10,000 people visit our websites every day. We know from the feed-back we receive just how much we are valued by people trying to beat cancer.
We believe you can increase your personal odds of cancer survival by taking simple health-enhancing steps and adding both complementary cancer therapies and alternative cancer therapies into your mix of treatments.
For example, Hyperbaric Oxygen, curcumin, calorie restriction, melatonin, probiotics and whole body hyperthermia have all been shown in research to make chemotherapy work better. It kills more cells! The research is covered on this website. Surely it makes a lot of sense to use them in your personal cancer treatment programme?
We have a complete review of Immunotherapy telling you the accurate figures and what to watch out for. We tell you what is working and when two new drugs have been used, rather than one. Its a new, emerging and alternative cancer therapy, but not fully there yet!
Go to: A complete review of Immunotherapy
Then we have an article on how to improve the success of your radiotherapy (and reduce the potential side-effects) – all by adding complementary therapies. Our Guidelines on Diet and Exercise can be found through this link:
Go to: CANCERactive Guidelines on Diet and exercise
Our recommended anti-cancer diet is the colourful Mediterranean Diet (with its focus on the French paradox):
Go to: The Rainbow Diet
Like Hippocrates, we believe all cancer begins in the gut and that gut problems, yeast, viral and parasite infections are common constituents of cancer.
Go to: All cancer begins in the gut
But if you just want to look at the most comprehensive list of Complementary Therapies you can find it here:
Go to: CANCERactive Complementary and Integrative cancer therapies
And if you want alternative cancer therapies start here:
Go to: CANCERactive Alternative cancer therapies
Finally, if you want all this put together for you in one simple plan, why not look into having a Personal Prescription?
Go to: Personal Prescriptions with Chris Woollams
We don’t take one penny from any Pharmaceutical company, cancer clinic or supplements company. We have no vested interest. We just want to see you beat cancer.
"If you are already thinking of supplementing with any of the above products, why not take a look at Our Natural Selection by clicking here."

The CANCERactive Difference:
Intelligent Information. Independent Voice.
IMPORTANT INFORMATION
|
*Cancer (and its related illnesses) are very serious and very individual diseases. Readers must always consult directly with experts and specialists in the appropriate medical field before taking, or refraining from taking, any specific action.
This web site is intended to provide research-based information on cancer and its possible causes and therapies, so that you can make more informed decisions in consultation with those experts. Although our information comes from expert sources, and is most usually provided by Professors, scientists and Doctors, our easy-to-understand, jargon-free approach necessitates that journalists, not doctors, write the copy. For this reason, whilst the authors, management and staff of CANCERactive, icon, and Health Issues have made every effort to ensure its accuracy, we assume no responsibility for any error, any omission or any consequences of an error or omission. Readers must consult directly with their personal specialists and advisors, and we cannot be held responsible for any action, or inaction, taken by readers as a result of information contained on this web site, or in any of our publications. Any action taken or refrained from by a reader is taken entirely at the readers own instigation and, thus, own risk.
|